July 2014 Issue
Vitamin D’s Role in Health — Deterministic or Indeterminate?
By Stephanie Dunne and Jenna A. Bell, PhD, RD
Today’s Dietitian
Vol. 16 No. 7 P. 48
Suggested CDR Learning Codes: 2000, 2020, 2090, 4030; Level 2
Take this course and earn 2 CEUs on our Continuing Education Learning Library
Although the name suggests otherwise, vitamin D isn’t a vitamin because it’s not an essential element of the diet. Rather, it’s a prohormone synthesized by the skin when it’s exposed to ultraviolet B (UVB) radiation.1 Yet despite the body’s ability to produce vitamin D and its availability in some foods, estimates indicate that 50% of children and adults worldwide have insufficient amounts of vitamin D in their bodies.2 From Canada to South Africa and every latitude in between, vitamin D deficiency appears to be common, and it may be causing a wide range of health issues.2
This continuing education course explores how the body absorbs and metabolizes vitamin D, discusses its functions in the human body, explains how to evaluate appropriate blood levels based on the latest research, and identifies sources of the nutrient.
Absorption and Metabolism
Vitamin D comes in two major forms: vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). Primarily, vitamin D2 is manufactured and used to fortify foods, while vitamin D3 is synthesized in the skin and naturally available in some animal-based foods. Commercially manufactured supplements contain either form.3 Because these two forms have identical metabolism and function, the term “vitamin D” is used to represent both vitamins D2 and D3 unless specified.
Although vitamin D is available in both foods and supplements, sun exposure is the most significant source for most people.4 When UVB rays hit the skin, approximately 10% to 15% of the 7-dehydrocholesterol found in the skin is converted to pre–vitamin D3. In a thermal-dependent reaction, pre–vitamin D3 then is isomerized to vitamin D3 before being bound to vitamin D–binding protein and released into the circulating blood.1,5
Vitamin D3 then travels to the liver, where it’s hydroxylated to calcidiol, or 25-hydroxyvitamin D [25(OH)D]. Calcidiol then is carried to the kidneys and other tissues, where it’s enzymatically converted to its active form, calcitriol or 1alpha,25(OH)2D.5 The conversion from calcidiol to calcitriol primarily occurs in the kidneys but also can occur in muscle tissue; the cells of the colon, prostate, pancreas, lungs, skin, breasts, and brain; and the immune system.1,2,5
When people ingest vitamin D from food sources, the intestine’s epithelial cells absorb the vitamin D and carry it via chylomicrons through the lymphatic system and into the circulatory system.5 From the chylomicrons, vitamin D may be transferred to the vitamin D–binding protein and released into the liver, or it may stay in the chylomicron where it will be taken up by the liver, which is the last stop for the chylomicron after circulating in the body.1 Once in the liver, dietary vitamin D follows the same activation path as that produced from UVB rays by being hydroxylated into 25(OH)D and then into 1alpha,25(OH)2D.
Calcitriol is a self-limiting entity. High levels reduce the kidney’s production of 25-hydroxyvitamin D-1alpha-hydroxylase, which lessens the amount of calcidiol that’s converted to calcitriol.5 Calcitriol also upregulates the production of 25-hydroxyvitamin D-24-hydroxylase, an enzyme in the kidneys and other tissues that’s responsible for inactivating both calcidiol and calcitriol. Once vitamin D has been inactivated by being turned into either 24,25(OH)2D or calcitroic acid, it returns to the liver where it’s added to bile and excreted in the feces.1
Functions of Vitamin D
Since Polish physician Jerdrzei Sniadecki realized that rickets, the bone-deforming disease in children, could be prevented and cured with sunlight, vitamin D has been well established as an essential part of calcium and phosphorus homeostasis and therefore bone maintenance.2,3 Specifically, calcitriol increases calcium and phosphorus absorption from the intestine and prevents the kidneys from excreting calcium and phosphate. Calcitriol also stimulates preosteoclasts to mature into osteoclasts, which break down bone and release calcium and phosphate into the blood. In an effort to recover homeostasis, parathyroid hormone (PTH) triggers both of these mechanisms when serum calcium and phosphate levels have dropped too low.5,6
Since there are numerous vitamin D receptors throughout the body, it appears that the nutrient has many other functions beyond bone health.5 In fact, vitamin D directly or indirectly influences as much as 5% of the genes in the human genome.3 Also, between 200 and 600 genes are primary targets of vitamin D, as they’re directly involved with vitamin D receptors. As the direct effect, vitamin D may cause an increase or decrease in the expression of the target gene depending on the gene itself.1,7
In addition to genetic influences, vitamin D receptors are found in the membranes of many cells, including those in the brain, gonads, skin, vascular smooth muscle, and immune system. These receptors allow vitamin D to trigger secondary messengers within some cells, causing a rapid hormonelike response that doesn’t involve genetic changes.1,2,5
Few studies regarding vitamin D’s effect on various conditions have been randomized controlled trials. In fact, most studies have been observational and show correlation but can’t prove causation.4,6 Therefore, it’s possible that sociodemographic factors, lifestyle choices, and metabolic health are confounding factors in studies reporting vitamin D’s impact on health.4
That being said, the epidemiologic evidence and scientific studies showing that vitamin D’s effects go beyond bone health are increasing. For example, infants who received 2,000 IU/day of a vitamin D supplement had an 88% lower risk of developing type 1 diabetes by the age of 32, and normotensive children given 2,000 IU/day had significantly lower arterial wall stiffness after 16 weeks compared with children who were given only 400 IU/day.6
Another study showed that children given 1,200 IU of vitamin D per day for four months during the winter reduced their risk of an influenza A infection by more than 40%.2 And pregnant women deficient in vitamin D seem to be at greater risk of preeclampsia and cesarean section.6
The following are some of the ways vitamin D appears to maintain health1-5:
• Cancer: suppresses the proliferation of and stimulates the differentiation and apoptosis of some kinds of cancer cells, especially breast, prostate, and colon;
• Diabetes: triggers the transcription of the insulin receptor gene in peripheral target cells and activates the release of insulin from the pancreas’ beta cells;
• Cardiovascular disease: decreases PTH levels and the release of renin by the kidneys, which helps reduce blood pressure;
• Muscular function: increases calcium uptake by muscles and stimulates the intracellular release of calcium within the muscle to maintain appropriate muscle contraction;
• Immunity: upregulates macrophages’ production of cathelicidin, a protein that helps them fight conditions such as upper respiratory infections and tuberculosis;
• Parkinson’s disease, Alzheimer’s disease, depression, and schizophrenia: prevents the loss of dopaminergic neurons in the brain; and
• Multiple sclerosis, rheumatoid arthritis, Crohn’s disease, and type 1 diabetes: suppresses the autoimmune response.
Although scientific studies haven’t proven these effects, they’re considered plausible because of the interaction between the regulating mechanisms of these conditions and vitamin D levels. For example, PTH modulates vasoconstriction and blood pressure, and is the principal activator of the renal gene CYP27B1. PTH concentrations rise when serum levels of vitamin D drop too low, which increases calcidiol activation.1,8 On the other hand, cytokines are responsible for the upregulation of the gene CYP27B1 in macrophages and the subsequent impact of calcitriol on the immune system.1
Recommended Blood Levels
Calcidiol, the inactive form of vitamin D, is the most abundant form found in the blood and the one used as a primary marker of vitamin D status.5 Calcitriol isn’t considered a useful marker of vitamin D levels because it can remain within normal limits even when hypovitaminosis D is present. In addition, low calcitriol levels may be the result of kidney disease rather than an indicator of vitamin D synthesis or intake.9
Normal circulating levels of calcidiol reach 25 to 200 nmol/L, although it’s uncommon to see average values in population studies above 30 to 32 nmol/L.1,6 The Institute of Medicine (IOM) defines vitamin D deficiency as a serum calcidiol level below 20 nmol/L, indicating that this is the minimum advisable level for the general population and not for any populations with special considerations related to vitamin D.10
However, some experts say this level was chosen based solely on vitamin D’s effect on bone health, even though evidence of osteomalacia in adults still may be seen until serum levels reach at least 30 nmol/L.2 Moreover, 30 nmol/L appears to be the threshold for preventing hip and nonvertebral fracture, and PTH levels plateau between 30 and 40 nmol/L, indicating there still is a risk of bone remodeling until this level of serum calcidiol is achieved.6
The IOM also indicates that vitamin D insufficiency occurs when serum calcidiol levels drop below 50 nmol/L. If a person’s vitamin D level is insufficient but not deficient, it means the person’s risk of developing osteomalacia or another problem with bone mineralization is higher. Because of the seasonal variations seen in vitamin D status and bone resorption, a serum level of at least 80 nmol/L may need to be obtained in the summer to ensure serum levels don’t fall below 50 nmol/L during the winter months.5
Beyond bone health, some experts suggest that a serum vitamin D level of more than 75 nmol/L is necessary to positively impact long-latency diseases.8 Specifically, at 80 nmol/L, vitamin D no longer is the limiting factor for calcium absorption from the intestine. At 90 to 100 nmol/L, lower extremity function, dental health, and blood pressure are optimized, while the risk of fall, fracture, cardiovascular disease, all-cause mortality, and colorectal cancer are reduced.5,11 In fact, falls weren’t reduced in people aged 65 and older when serum vitamin D levels were below 60 nmol/L.11 Obviously, these suggested levels are significantly higher than the levels currently recommended by the IOM.
The IOM indicates that a serum 25(OH)D level higher than 125 nmol/L puts a person at increased risk of vitamin D excess, which can lead to hypercalcemia and overcalcification of bone, soft tissues, the heart, and the kidneys.7,8 Most studies in children and adults have shown that hypercalcemia doesn’t occur even with serum vitamin D levels of 150 nmol/L, and some studies have indicated serum calcium remained within normal limits until serum calcidiol levels were higher than 240 nmol/L.6,7 Specifically, in a meta-analysis of 28 trials, average serum calcium didn’t change even when calcidiol was higher than 600 nmol/L. In these studies, hypercalcemia was observed in isolated situations, such as when a participant had primary hyperparathyroidism or Williams syndrome or when high calcium intake coincided with high vitamin D intake. The hypercalcemia often resolved on a second test, indicating that the initial high serum calcium likely resulted from a contributing factor other than high vitamin D intake.2,6,11
It’s worth noting that many options exist for measuring the amount of calcidiol in the blood: chemiluminescence immunoassay, radioimmunoassay, liquid chromatography, high-performance liquid chromatography, and liquid chromatography–tandem mass spectrometry. However, the various tests return different results. For example, in one study, the number of participants with normal calcidiol levels was 19.9% with chemiluminescence immunoassay and 31.7% with liquid chromatography–tandem mass spectrometry.8 Also, the testing reagents may respond differently to vitamin D2 metabolites than to those from vitamin D3.
The problem of inconsistency should improve since reference materials from the US National Institute of Standardization were made available in 2010, although standardized reporting and interlaboratory comparison still are needed.9 However, the Endocrine Society indicates that all methods for vitamin D measurement are valid as long as the reference range for the chosen method indicates the target calcidiol level is above the current minimum recommendation.6
Hypo- and Hypervitaminosis D
With all of the proven and possible effects, it’s clear that vitamin D is required for good health. However, various factors can contribute to too low or too high vitamin D levels and should be taken into consideration when RDs counsel clients or patients on whether they should be tested.
Primarily, hypovitaminosis D results from lifestyle changes that have occurred in the past few decades.9 Reduced sun exposure from clothing, more time spent indoors, and increased sunscreen use all inhibit the skin’s synthesis of vitamin D.5 Children and adolescents’ reduced consumption of vitamin D–fortified milk also contributes to widespread vitamin D deficiency.6
In addition to diet and sun exposure, other factors related to health and a healthful lifestyle also seem to affect vitamin D levels. Lower levels of vitamin D have been observed in people with the metabolic syndrome, particularly based on their HDL cholesterol levels and waist circumference.4 One study found that waist circumference accounted for 1.9% of the variation in vitamin D status, while BMI explained none of the difference, indicating that perhaps abdominal adiposity specifically, and not obesity generally, may be a factor in developing hypovitaminosis D.8
Adiposity’s impact on vitamin D may be explained by the increased PTH levels often measured in people who are obese or because adipocytes sequester vitamin D.4,6 As a result, people with larger amounts of adipose tissue may be able to increase their serum calcidiol levels only one-half as much as people with less fat mass when given similar doses of vitamin D.6 Also, higher vitamin D levels have been observed in those who moderately consumed alcohol, didn’t smoke, and had normal blood pressure and serum lipid profiles. These differences were seen even when taking into account the difference in vitamin D levels that’s expected based on age, sex, and the month of blood sampling.4
For babies and children, breast-feeding with no vitamin D supplementation has been associated with the risk of deficiency because human breast milk and colostrum contain very little vitamin D. Preliminary data suggest that when lactating women take a daily vitamin D supplement containing 4,000 to 6,000 IU, they transfer enough vitamin D via breast milk to meet their baby’s requirements.6
Regarding uncontrollable factors, aging and skin pigmentation contribute to lower levels of vitamin D. As a person ages, the skin’s ability to produce vitamin D when exposed to UVB rays diminishes.4 It’s estimated that people who are older than 60 can create only one-half as much vitamin D as those who are younger than 20 when exposed to the same amount of sunlight.12
People with darker skin pigmentation are at risk of having lower vitamin D levels due to competition for UVB ray absorption caused by melanin.5,13 Those with a naturally dark skin tone require three to five times longer sun exposure to make the same amount of vitamin D in the skin as do those with a very light skin tone.6
Certain conditions also can negatively affect vitamin D status. Conditions that produce granulomas (small areas of inflammation caused by tissue injury) can increase the conversion of calcidiol to calcitriol, which can lead to hypercalciuria and hypercalcemia.6 Granulomatous disorders include sarcoidosis, tuberculosis, chronic fungal infections, and some lymphomas. Some malabsorption syndromes, such as cystic fibrosis and inflammatory bowel disease, also can cause decreased absorption of dietary vitamin D.2
In addition to some medical conditions, various medications can affect vitamin D levels. Among the drugs that may cause increased vitamin D catabolism are anticonvulsants, glucocorticoids, antifungals such as ketoconazole, and highly active antiretroviral therapy for AIDS. Taking these medicines may require individuals to obtain two to three times more than the recommended amount of vitamin D for their age group to reach the recommended level of serum calcidiol.5 In contrast, exogenous hormones have been shown to increase vitamin D levels, possibly because of the increased concentration of vitamin D–binding protein.8
Although rare, genetic mutations can lead to rickets or osteomalacia because of the impact on vitamin D metabolism and function. As with the production of all human enzymes, certain genes are responsible for providing the instructions for creating the enzyme. As illustrated in Table 1, there are multiple genes involved in creating the enzymes responsible for vitamin D activation and inactivation. Additional genes are responsible for creating the proteins that allow cells to absorb vitamin D from the blood. If one or more of these genes don’t produce the necessary enzymes or vitamin D receptors, the same outcomes as seen in vitamin D deficiency can result.1
Table 1: Important Genes and Their Enzymes Involved in Vitamin D Metabolism1
Gene |
Enzyme |
Location |
Conversion |
CYP27A1 |
Vitamin D-25-hydroxylase |
Liver |
Vitamin D2 or D3 à calcidiol [25(OH)D] |
CYP2R1 |
Vitamin D-25-hydroxylase |
Liver |
Vitamin D2 or D3 à calcidiol [25(OH)D] |
CYP27B1 |
25-hydroxyvitamin D-1alpha-hydroxylase |
Kidney and other tissues |
Activation: Calcidiol [25(OH)D] à calcitriol [1alpha,25(OH)2D] |
CYP24A1 |
25-hydroxyvitamin D-24-hydroxylase |
Kidney and other tissues |
Inactivation: Calcitriol or calcidiol à 24,25(OH)2D or calcitroic acid |
The pathology of genetic mutations that lead to rickets or osteomalacia often is described as vitamin D–dependent rickets or pseudo–vitamin D deficiency rickets because the problem lies with vitamin D activation or absorption rather than being a true vitamin D deficiency.5 The following are genetic mutations that influence vitamin D function1,5:
• CYP27A1: causes a bile acid and lipid metabolism disorder and may result in low calcidiol levels;
• CYP2R1: results in low levels of vitamin D-25-hydroxylase and calcidiol;
• CYP27B1: marked by decreased levels of calcitriol and normal serum levels of calcidiol;
• Vitamin D receptor coding gene: marked by increased calcitriol levels;
• Hormone response element–binding protein: limits vitamin D receptor binding; and
• CYP24A1: marked by increased serum vitamin D and calcium.
Although hypovitaminosis D is more common, hypervitaminosis D can occur and primarily results in hypercalcemia and overcalcification of bone, soft tissues, the heart, blood vessels, and kidneys, as mentioned previously.7,8 Symptoms of hypervitaminosis D include anorexia, dry mouth, a metallic taste, nausea, vomiting, constipation, and diarrhea. With long-term oversupplementation, additional symptoms may include polydipsia, depression, headache, drowsiness, and weakness.
Elevated vitamin D levels may cause abnormally elevated serum values for blood urea nitrogen, creatinine, aspartate aminotransferase, alanine aminotransferase, and cholesterol and elevated urinary values of calcium, phosphorus, and albumin. Toxicity also can cause poor growth in children.14
Because the cost of testing can be high and many people seem to be deficient because of insufficient sun exposure and low dietary intake, most experts don’t recommend population testing for vitamin D status. In fact, the test results for most people are expected to indicate deficiency unless people recently have been exposed to the sun and/or are taking a vitamin D supplement.
However, there are some situations for which testing is warranted and recommended. Situations for which vitamin D testing is indicated to confirm hypo- or hypervitaminosis D so recommendations for correction can be made, as appropriate, include the following2,3,6:
• bone diseases (eg, rickets, osteomalacia, osteoporosis);
• chronic kidney disease or nephrotic syndrome;
• hepatic failure;
• malabsorption syndromes (eg, cystic fibrosis, inflammatory bowel disease, bariatric surgery, radiation enteritis, Whipple’s disease, celiac disease);
• primary hyperparathyroidism;
• when taking certain medications (eg, antiseizures, glucocorticoids, highly active antiretroviral therapy, exogenous hormones);
• in older adults with a history of falls or nontraumatic fractures;
• in children and adults who are obese;
• granulomatous disorders (eg, sarcoidosis, tuberculosis, histoplasmosis, coccidiomycosis, berylliosis, some lymphomas);
• hereditary phosphate-losing disorders;
• pseudo–vitamin D deficiency rickets; and
• vitamin D–resistant rickets.
Recommended Intake
In 2011, the IOM published Dietary Reference Intakes for Calcium and Vitamin D to update the information provided in its 1997 report.3 With new data and the ability to integrate older data sets, the IOM established Adequate Intake levels for infants and Estimated Average Requirement and Recommended Dietary Allowance levels for children and adults (see Table 2).
Table 2: Daily Vitamin D Dietary Reference Intakes for All Life Stages3
Life Stage |
Adequate Intake |
Estimated Average Requirement |
Recommended Dietary Allowance |
Infants: 0 to 12 months |
400 IU |
|
|
Children: 1 to 8 years |
|
400 IU |
600 IU |
Adolescents: 9 to 18 years |
|
400 IU |
600 IU |
Adults: 19 to 70 years |
|
400 IU |
600 IU |
Adults: 70+ years |
|
400 IU |
800 IU |
Pregnancy/lactation |
|
400 IU |
600 IU |
Note that 100 IU = 2.5 mcg.
Because the amount of vitamin D the skin produces when exposed to UVB rays is influenced by many factors, the IOM is unable to recommend an amount of sun exposure that would ensure adequate vitamin D production for all people.3 As such, the Dietary Reference Intakes are limited to dietary intake and assume minimal sun exposure. In addition, the report indicates that the values are based on dose-response relationships for bone health only, as data are inconclusive regarding vitamin D’s effect on other health factors.
The IOM has concluded there’s no evidence that serum calcidiol levels higher than 50 nmol/L provide additional benefits to bone health. It predicts that a daily intake of 600 IU will result in an average serum calcidiol level of 63 nmol/L for children and adults of all ages in northern latitudes during the winter, when sun exposure likely is the lowest for the year.3,5
In contrast to the IOM’s recommendation, the Endocrine Society indicates that individuals may need a dietary intake of as much as 1,500 IU of vitamin D per day to ensure serum calcidiol consistently is higher than 30 nmol/L. This indication is based on the society’s estimation that people of normal weight need 100 IU/day to increase their serum calcidiol level by 1 ng/mL, and that most people are deficient in vitamin D.6
In addition, a review by Bischoff-Ferrari and colleagues found that only 66% of adults can achieve a serum calcidiol level of at least 50 nmol/L when following the IOM’s Estimated Average Requirement for vitamin D. Most healthy adults of all ages achieved what some consider to be the optimal calcidiol level of 75 to 110 nmol/L when consuming 1,800 to 4,000 IU/day for at least 42 days.11
As mentioned previously, many factors determine individuals’ vitamin D status based on their ability to absorb, metabolize, and utilize it. After assessing for conditions that may contribute to hypo- or hypervitaminosis D and the amount of sun exposure that will contribute to vitamin D synthesis, an individualized recommendation for dietary intake can be established using the Recommended Dietary Allowances as a guideline.
Sources of Vitamin D
Sunlight is the most efficient source of vitamin D for people. An adult wearing a bathing suit with enough sun exposure to cause a slight pinkness to the skin gets the same amount of vitamin D as does one who ingests 20,000 IU of vitamin D.2 In addition, vitamin D produced by the skin seems to stay in the body longer than does vitamin D from dietary sources or supplements.6
However, warnings from health organizations that excess sun exposure causes skin cancer has resulted in many people wearing extra clothing and using sunscreen while outside, which severely reduces the amount of vitamin D produced by the skin. To put it in perspective, using an SPF 30 sunscreen reduces the body’s ability to synthesize vitamin D by at least 95%.6
In addition to sunscreen and clothing, the angle of the sun influences how much vitamin D can be produced from sun exposure. The zenith angle of the sun represents the angle at which the rays of the sun hit the earth, and it’s affected by latitude, season, and time of day, as demonstrated in Image 1.6
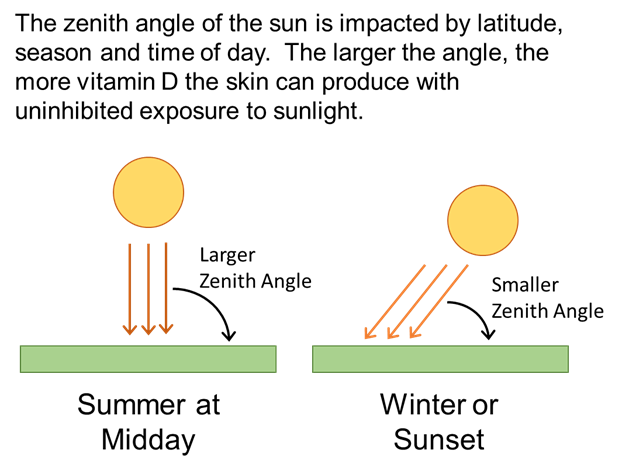
As an example, people at 52˚N latitude get about one-half of the annual UVB rays as do people at 40˚N latitude.12 For people above 33˚N latitude and below 33˚S latitude, the angle of the sun is too low during the winter months to produce any vitamin D in the skin, regardless of duration of exposure.6 The smaller the zenith angle of the sun, the less vitamin D can be produced by the skin.
Skin cancer is a serious health risk related to sun exposure, and precautionary measures should be taken. However, occupational and sensible sun exposure hasn’t been shown to significantly increase the risk of nonmelanoma skin cancer.2 Also, sensible sun exposure results in higher vitamin D levels, which may decrease the incidence of melanoma due to growth inhibition and apoptosis promotion.12
Finally, warnings about skin cancer don’t take into account that more deaths occur each year from internal cancers and disorders potentially associated with low vitamin D levels than from high UV light exposure (63,000 vs. 10,000 annually).12
Of course, given that many people can’t generate enough vitamin D from sun exposure due to factors such as latitude, indoor lifestyle, and skin pigmentation, dietary sources also should be considered. As mentioned, dietary sources include both vitamin D3 from animal sources and vitamin D2 from plant sources.5
Although some studies have indicated that vitamin D3 has a higher potency in the body than does vitamin D2, not all studies have reached the same conclusion, and differentiation hasn’t proven to be necessary.1,6 As indicated in Table 3, foods that are naturally high in vitamin D include salmon, sardines, herring, and other oily fish as well as cod liver oil, egg yolks, and sun-exposed mushrooms.1,2
Table 3: Selected Food Sources of Vitamin D15
Food |
Serving Size |
Approx. IU/Serving |
Cod liver oil |
1 T |
1,360 |
Raw maitake mushrooms, diced |
1 cup |
786 |
Swordfish, cooked |
3 oz |
706 |
Salmon, sockeye, cooked |
3 oz |
447 |
Fortified skim milk |
1 cup |
120 |
Fortified orange juice |
1 cup |
100 |
Whole Grain TOTAL cereal |
3/4 cup |
100 |
Fortified nonfat yogurt with fruit |
6 oz |
88 |
Tuna, canned in water, drained |
3 oz |
68 |
Fortified margarine |
1 T |
64 |
Egg, chicken, whole, scrambled |
1 |
44 |
Note that 100 IU = 2.5 mcg.
In the United States, many foods are fortified with vitamin D manufactured by UV irradiation of ergosterol produced by yeast. Fortified foods contain approximately 100 IU per serving and include many dairy products, such as milk, yogurt, butter, and cheese; orange juices; margarines; breakfast cereals; and infant formulas.2
Vitamin D is available in commercial supplements and some multivitamins or in pharmaceutical formulations. Physicians can prescribe a liquid supplement with 8,000 IU/mL for infants and younger children or a gelatin capsule with 50,000 IU for older children and adults. Vitamin D supplements are available with as little as 400 or as many as 50,000 IU per serving.
In addition to straight vitamin D supplements, many multivitamins contain 400 to 1,000 IU of vitamin D, and many commercial calcium supplements also contain vitamin D because of the relationship between the two micronutrients. Supplementation is effective at maintaining serum levels when taken at various intervals, including daily, weekly, and every four months.6 Vitamin D supplements and multivitamins can be taken with or without food.14
The Challenges of Putting It Into Practice
In recent years, the prohormone known as vitamin D has been getting attention for its potential role in a host of health issues, from autoimmune diseases to cancer. Despite mounting data from observational studies, the IOM has reported that conclusive evidence from randomized controlled trials is insufficient to declare that vitamin D plays a definitive role in conditions beyond those related to bone health.3 While the Endocrine Society and other experts agree that the evidence still is building, they argue that the potential for benefit outweighs the risk of harm in recommending higher vitamin D intake levels.5 As a result, RDs should be aware that an optimal serum calcidiol level is higher than 30 nmol/L and can be as high as 75 nmol/L without causing adverse effects and potentially protecting the person from long-latency diseases.3,5
To reach an appropriate serum calcidiol level, the IOM recommends a daily vitamin D intake of 400 IU in the first year of life, 600 IU until the age of 70, and 800 IU from age 70 onward.3 However, given the many genetic, environmental, and metabolic factors that influence vitamin D status, RDs may need to counsel clients or patients to ingest two to three times the recommended amount to achieve the desired result. The Endocrine Society suggests that children and adolescents may need up to 1,000 IU/day and people older than 18 may need 1,500 to 2,000 IU/day to consistently achieve blood calcidiol levels higher than 30 nmol/L.6 RDs may be concerned that the higher intake levels will cause toxicity in the form of hypercalcemia, but that toxicity typically isn’t seen until intake exceeds 10,000 IU/day for several months.2,6
In waiting for future research to clarify vitamin D’s role in the human body and the necessary intake to achieve the required levels, RDs should use the Recommended Dietary Allowance as the minimum intake that ensures their clients and patients can maintain bone health. Then, when individualizing the recommendation, RDs should consider lifestyle, environmental factors, malabsorption issues, medication use, genetic mutations, and other health conditions that can increase or decrease skin synthesis, metabolism, and usability of vitamin D.
— Stephanie Dunne is a graduate student in nutrition and a dietetic intern at Lehman College in the Bronx, New York.
— Jenna A. Bell, PhD, RD, is senior vice president and director of food and wellness at Pollock Communications in New York City; the 2013-2014 chair of the Sports, Cardiovascular, and Wellness Nutrition Dietetic Practice Group; and a coauthor of Energy to Burn: The Ultimate Food & Nutrition Guide to Fuel Your Active Lifestyle.
Learning Objectives
After completing this continuing education course, nutrition professionals should be better able to:
1. Assess vitamin D’s life cycle in the body.
2. Evaluate vitamin D’s involvement in various aspects of health.
3. Determine recommended intakes of vitamin D.
4. Distinguish the sources of vitamin D.
CPE Monthly Examination
1. Vitamin D is considered to be which of the following?
a. Vitamin
b. Hormone
c. Prohormone
d. Antioxidant
2. Which of the following genetic mutations can result in normal levels of 25-hydroxyvitamin D [25(OH)D] and low levels of 1alpha,25(OH)2D?
a. CYP27A1
b. CYP27B1
c. CYP2R1
d. CYP24A1
3. Vitamin D testing specifically is recommended for which of the following groups?
a. People with liver failure
b. People who live north of 45˚N latitude
c. All adults older than 65
d. Everyone
4. Which of the following is the active form of vitamin D in the body?
a. Calcitroic acid
b. Calcidiol
c. Calcitriol
d. 24,25(OH)2D
5. Beyond bone health, vitamin D seems to help maintain health in which of the following ways?
a. Maintaining kidney function
b. Supporting muscle growth
c. Promoting weight loss
d. Suppressing the autoimmune response
6. Which of the following foods has the highest content of vitamin D per serving?
a. Cod liver oil
b. Sun-dried mushrooms
c. Swordfish
d. Fortified skim milk
7. The sun is too low during the winter months to produce any vitamin D in the skin above and below which north/south parallel?
a. 20˚
b. 33˚
c. 40˚
d. 52˚
8. Vitamin D is associated with bone health because it does which of the following?
a. Stimulates osteoblasts
b. Increases phosphorus excretion
c. Reduces parathyroid hormone release
d. Increases calcium absorption from the intestine
9. The Institute of Medicine identifies vitamin D deficiency as serum calcidiol levels below which of the following levels?
a. 15 nmol/L
b. 20 nmol/L
c. 32 nmol/L
d. 50 nmol/L
10. Each serving of foods fortified with vitamin D contain approximately which of the following amounts?
a. 2.5 mcg (100 IU)
b. 25 mcg (1,000 IU)
c. 40 mcg (1,600 IU)
d. 100 mcg (4,000 IU)
References
1. Jovicic S, Ignjatovic S, Majikic-Singh N. Biochemistry and metabolism of vitamin D. J Med Biochem. 2012;31(4):309-315.
2. Holick MF. The d-lightful vitamin D for health. J Med Biochem. 2013;32(1):1-10.
3. Ross AC, Taylor CL, Yaktine AL, Del Valle HB (eds). Dietary Reference Intakes for Calcium and Vitamin D. Washington, D.C.: National Academy Press; 2011.
4. Jaaskelainen T, Knekt P, Marniemi J, et al. Vitamin D status is associated with sociodemographic factors, lifestyle and metabolic health. Eur J Nutr. 2013;52(2):513-525.
5. Battault S, Whiting SJ, Peltier SL, Sadrin S, Gerber G, Maixent JM. Vitamin D metabolism, functions and needs: from science to health claims. Eur J Nutr. 2013;52(2):429-441.
6. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911-1930.
7. Carlberg C, Seuter S, de Mello VDF, et al. Primary vitamin D target genes allow a categorization of possible benefits of vitamin D3 supplementation. PLoS ONE. 2013;8(7):e71042. doi:10.1371/journal.pone.0071042
8. Kuhn T, Kaaks R, Teucher B, et al. Dietary, lifestyle, and genetic determinants of vitamin D status: a cross-sectional analysis from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Germany study. Eur J Nutr. 2013;Epub ahead of print.
9. Vogeser M, Seger C. Vitamin D—challenges in diagnosing and monitoring of hypovitaminosis D. J Med Biochem. 2012;31(4):316-325.
10. Rosen CJ, Abrams SA, Aloia JF, et al. IOM committee members respond to Endocrine Society vitamin D guideline. J Clin Endocrinol Metab. 2012;97(4):1146-1152.
11. Bischoff-Ferrari HA, Shao A, Dawson-Hughes B, Hathcock J, Giovannucci E, Willett WC. Benefit–risk assessment of vitamin D supplementation. Osteoporos Int. 2010;21(7):1121-1132.
12. Godar DE, Pope SJ, Grant WB, Holick MF. Solar UV doses of adult Americans and vitamin D3 production. Dermatoendocrinol. 2011;3(4):243-350.
13. Moreno-Reyes R, Carpentier YA, Boelaert M, et al. Vitamin D deficiency and hyperparathyroidism in relation to ethnicity: a cross-sectional survey in healthy adults. Eur J Nutr. 2009;48(1):31-37.
14. Pronsky ZM, Crowe JP. Food-Medication Interactions. 17th ed. Birchrunville, PA: Food-Medication Interactions; 2012.
15. National Nutrient Database for Standard Reference Release 26. US Department of Agriculture website. http://ndb.nal.usda.gov/ndb/search/list. Accessed October 26, 2013.